We believe our HEART model outlined below is the most effective way of both supporting professionals and affecting meaningful change / Really Making A Difference.

Introduction
Between 2012 – 2016 whilst working with members of the Aboriginal Community in Victoria Australia, Gavin developed a model which provided a framework and road map to assess complex / developmental trauma and successfully facilitate healing and recovery.
After completing training in Compassion Focused Therapy with Paul Gilbert in 2018, Gavin further developed his model to incorporate a Compassion Focused Lens, renamed it the HEART approach and introduced it to Westminster Children’s Services.,
Since its introduction into Westminster, HEART has proven to be successful in enabling Intensive Support and Edge of Care teams and services for Vulnerable Young Adults aged 18-25, to promptly assess and successfully respond to the needs of the ‘at risk’ and vulnerable.
The model is best understood if we break it down to four distinct parts which should ideally be introduced sequentially. However, given the model is designed to be flexible n and adaptable, the parts outlined below can be used as a guide. The final decision on sequencing, will be down to the Practitioner and their Supervisor.
Ideally part 2 and 3 should be delivered in a single session which often requires up to 2 ½ to 3 hours. Whilst this seems unrealistic, in practice it works well however in cases where families can not commit to this duration part three should be delivered as soon as possible after completion of part 2.
Please see below for a breakdown of the model.
Part 1:
Relationship Building Stage / Solution Focused Brief Therapy (SFBT)
The HEART prioritises the building of secure ‘therapeutic relationships’ between the practitioner, child / young person and their family characterised by the development of a mutually respectful and trusting connection.
The sense of safety that emanates from this “therapeutic relationship” enables conversations about historical exposure to Adverse Childhood Experiences (ACEs) which are the starting point for engagement, healing, and recovery.
The practitioner will use techniques from Solution Focused Brief Therapy (SFBT) to facilitate the child/young person and their family to identify best hopes and desired outcomes for the future, to agree goals to work toward and to co-construct a care plan.
Part 2:
Trauma Informed Mapping Exercise (TIME)
The Trauma Informed Mapping Exercise (TIME) is a psychotherapeutic intervention delivered as part of a partnership approach with the referred child’s parent(s)/carer(s).
The process involves the construction of a genogram and a timeline of significant events in a child’s life from conception to the present day which facilitates understanding of exposure to adverse childhood experiences (ACEs). The TIME then utilises a combination of functional analysis and attachment, child development and trauma theories to inform reflection on the experiences of the child.
This process is facilitated in a way that supports parents/carers to understand and accept the concept of developmental or complex trauma without internalising any blame or shame. This enables parents to concede their child is not ‘mad or inherently bad’ and that by engaging in specific targeted therapeutic interventions, their relationships can be repaired, and their child (ren) will be able to overcome their difficulties and achieve their full potential.
The child /young person does not attend the TIME as it is important that the parent (s) are able to share their story / feelings / emotions etc. without the fear of upsetting their child. Given the process is often emotionally charged and results in parents sharing raw and very honest stories, Practitioners also need the opportunity to reflect on how to appropriately present and reframe the information to and contain the emotions of the child prior to including them in the process.
Additionally, too many professionals with whom there is no relationship often present a barrier to parents being honest and feeling able to share what they may previously have considered as untellable. For this reason, only the key worker and the parents participate in the process. The voice of the child is ‘heard’ via their later participation in a child centred assessment process and child friendly version of the TIME as well as during subsequent Therapeutic Life Story Work and targeted Solution Focused activities where they share their thoughts and feelings on their life to date and reflect on their ‘best hopes’ for their future.
The key to the success of the TIME is that it is strengths based and facilitated in a non- judgemental way and at the pace of the parent / carer. This promotes the development of positive relationships and reduces the likelihood of parents feeling blamed or shamed which encourages parental engagement in the process and especially in the co-construction of their family care plan.
Both the genogram and timeline are completed in a real time session and all the information is provided by the parent / carer. This is important as it is the parent’s story / narrative and not that recorded on historical case notes. The timeline starts at the point the parents meet and continues to the current time to develop an understanding of the child’s experience and degree of exposure to any Adverse Childhood Experiences (ACEs). The line will include all significant events including:
- Mothers physical and emotional support prior to, during and post birth.
- Impact of birth / support on mother’s emotional wellbeing / mental health.
- Early childhood development & milestones.
- Quality of early parent child connection including provision of structure, routine, nurture.
- Summary of any concerns raised by staff from all schools attended.
- Any significant hospital visits and health care issues including episodes of self-harm and indications of emotional wellbeing /mental health difficulties including diagnoses and presentations.
- Any police call outs.
- Any periods of family conflict including controlling and or abusive behaviours and arguments from the point of the parents first meeting until the present day and any conflict to be scaled from 1-10 in terms of frequency and intensity and degree of child exposure.
- Quality of parent child relationship from day 1 onwards and when difficulties first arose.
- Quality of absent parent relationship with child / frequency of contact.
- Parent / carer relationships with subsequent romantic partners and impact of relationships on child including their understanding of why separations occurred.
Once the timeline is complete, the practitioner engages in reflective conversations focusing on strengths but ultimately facilitating the parent /carer to recognise without feeling ‘shamed’ that the child’s behaviours are the consequences of their exposure to identified ACES and that any repair to the filial relationship and change to any ‘challenging’ behaviours will require their commitment, involvement and participation.
Part 3:
Formulation via a Compassion Focused Lens
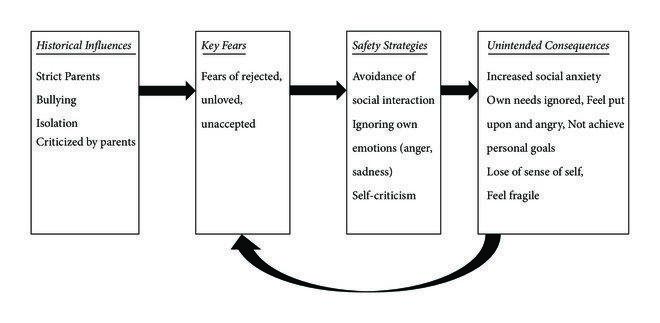
The HEART model utilises a Compassion Focused Therapy formulation to facilitate understanding of how exposure to historical influences such as adverse childhood experiences (ACEs) can result in a child developing fears.
These fears often include: a sense of being unloved, being unlovable and not being good enough, of being weak and powerless, of feeling unloved and unwanted and of feeling that when adults have control, it all goes wrong. Childrens fears are often overwhelming and left unchecked could result in paralysis. Consequently, to keep themselves safe from further harm, children often develop a range of unconscious behaviours. For example:
- In the case of children whose parents divorce, it is often the case a child will create an emotional suit of armour that prevents them from developing emotional connections with others to protect themselves from the pain of potential future loss, abandonment, and sense of being alone. Of course, the paradox of this approach is that the unintended consequence is often the very thing that the child was trying to protect themselves from.
- In the case of children exposed to domestic violence or parental neglect, it is often the case that children feel that their lack of control makes them vulnerable. To recompense they often become either oppositional and aggressive or overly compliant and appeasing in times of stress. Again, the paradox here is that their safety behaviours often create the very fears they are trying to avoid. This is especially true when their responses lead to school exclusions, involvement in the criminal justice system or of being controlled and exploited by others.
Please see table below for understanding of the CFT Formulation process.
Part 4:
Report, Recommendations, Family Plan and Interventions
The information gained from the TIME and the subsequent formulation exercise is then written up in a user-friendly report shared with the parent / carer. Following parental feedback, recommendations for targeted interventions are made and a ‘SMART’ Family Care plan is co constructed in partnership with the family. This plan is then reviewed at regular intervals until closure within 3-12 months of the completion of the agreed plan.
Targeted interventions include: (Please note Really MAD provides training in the highlighted interventions)
- Psycho education.
- Outcome measures including Trauma Symptoms Checklist for Children and Young People (TSCCYP) and the Strengths and Difficulties Questionnaires (SDQs).
- Risk Assessment / Risk Management plans.
- Child Young person assessment using TEEN TALK Assessment tools.
- Trauma Informed Mapping Exercise (For use with parents)
- Child TIME / Therapeutic Life Story Work (for use with children and young people).
- ‘Circle of Security / attachment informed’ parenting programme.
- Attachment Informed Games and Activities (informed by Theraplay)
- Non-Violent Resistance (NVR).
- HEART Feedback / Care Plan.
- Family Therapy / Family Meetings.
- Compassion Focused Practice.
- Compassion Focused Therapy.
- Emotional Wellbeing / Mindful Self Compassion.
- Emotional Freedom Technique (EFT)
- Therapeutic Mindful Drumming / Emotional regulation programme for Schools.

Make A Difference
Arrange a consultation for inspiring training to empower your team and promote wellbeing.